Elizabeth Kerner, MD
Plastic and Reconstructive Surgery

Common problems with enlarged breasts may include back pain, neck pain, difficulty exercising, bra strap grooving of the shoulders, as well as discomfort and rashes underneath the breasts. In addition to the physical problems associated with enlarged breasts, patients may be unhappy with the size of their breasts and their negative impact on appearance and self- image.
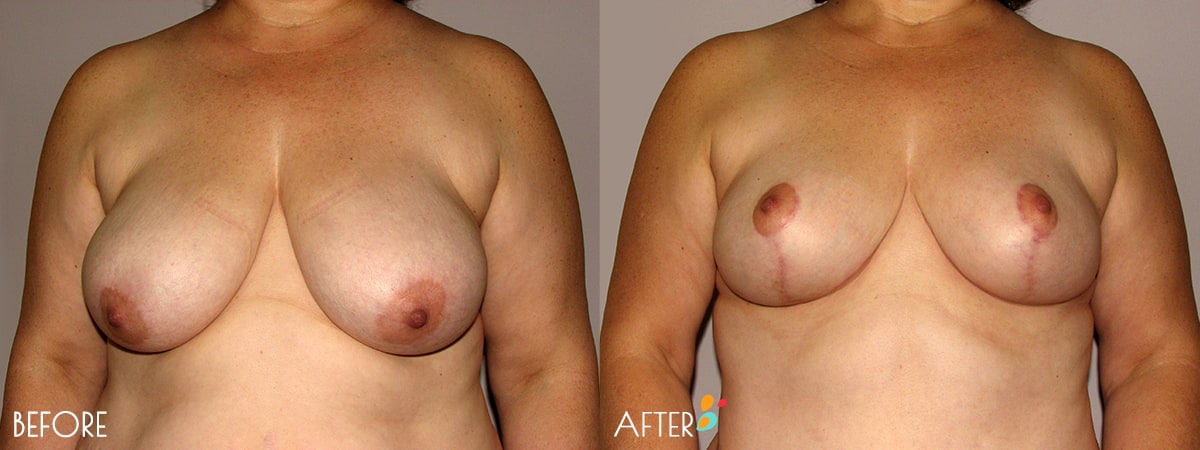
Breast reduction surgery reduces the size of the breasts while reshaping the breast contour and position. Patients will often experience significant improvement or complete resolution of their painful symptoms, and an improved body image and self esteem.
Breast surgery may be covered by insurance to alleviate shoulder and neck pain, rashes under the breasts, inability to exercise, and limitations in daily activity due to the weight and size of the breasts.
Reduction mammoplasty can be done on either an outpatient basis or with an overnight stay, and most operations take around four hours.
Postoperative pain following breast reduction surgery is typically well controlled using oral pain prescriptions. Patients typically plan for approximately a week of rest and down time after completing surgery, then two more weeks of somewhat restricted activity. Usually one can return to work after a week. Patients wear a supportive postoperative bra for approximately four weeks in order to allow for proper healing and the best outcome. Sutures are all dissolvable, and if drains are necessary, they are usually in for two or three days. The final breast shape and size is settled about four to five months after surgery.
“I’m Dr. Elizabeth Kerner, and welcome to Plain Talk About Plastic Surgery, your source for down to earth information and explanations about plastic surgery procedures and operations based on my three decades of experience.
Thank you for joining us for Episode Three. This is going to be all about Breast Reduction Surgery, a topic that is near and dear to my heart as I do so many of them and have for my 32 years in practice.
Let’s get started.
What is Breast Reduction Surgery?
Breast reductions are also called “Reduction Mammaplasty”. And that’s pretty easy to understand because “mama” comes from mammary gland and “reduction” would be to make the size smaller, therefore “Reduction Mammaplasty”.
For purposes of this podcast, I’m just going to call it “Reduction” as it gets to be awfully wordy if we continue to say “reduction mammaplasty”.
So what is a reduction mammaplasty?
It’s just a surgical means of reducing the size of the breast, and also uplifting. Lots of patients will ask me, well, if I’m having a breast reduction, does that mean I get to have a breast lift, or do I have to have that as a separate operation?
Breast reduction and breast lift are really the same thing. In lift, we don’t take out very much breast tissue or just a small amount. And in a breast reduction, we take out a lot more, but otherwise, the technical details of doing the operation are quite close.
Why Women Choose Breast Reduction Surgery
Why would women want to have a breast reduction?
The most common complaints that I hear would be neck, back, and shoulder pain, trouble buying clothes that fit because they gape in the middle. Difficulty with bras and then when you do get a bra that fits it has to be so supportive that you start to develop big shoulder strap grooving, and then difficulty with exercising.
Paying for Breast Reduction Surgery
Do you have to pay for breast reduction yourself? Is this considered a cosmetic operation?
That completely depends on your insurance company. For the longest time back in the 1990s, and up to about 2007 or 2008, breast reduction was almost always covered by insurance. As long as you had symptoms and had large breasts when we took a photograph, and met some fairly loose criteria, it would be covered by insurance.
However, now that insurances have become much more strict with what they’ll cover, there are very specific guidelines that we have to meet. These would include: you do have to have documented symptoms, and that’s usually neck, back and shoulder pain.
Depending on your insurance carrier, you may need to have failed what they call “conservative therapy”. That could be six weeks of physical therapy, or massage or you’ve had chiropractic treatment. All of that would be covered.
There are measurements that I need to take of your breast and I have to say satisfy the insurance company that your breasts would meet their minimum criteria. The most important part for the insurance though, is that I’m taking off sufficient amount of tissue in terms of weight to meet their minimum requirements.
For most patients, this is going to be around four to 500 grams per breast, which is about a pound per side. So you might reasonably ask, “How would I know how much I’m taking off?”
I just do it by feeling your breasts and getting an idea of the final volume that you would like to have and then see how much extra I’m going to be taking off. And after doing this for so many years, I’m pretty good about determining the weight that I’m feeling.
The insurance companies developed a scale called the Schnur Scale, it’s S-c-h-n-u-r, which was actually developed by a plastic surgeon back in the early 1990s. And Dr. Schnur came up with a sliding scale based on your body surface area. So if you are a tall woman who is very thin, then you’re going to require less tissue to be taken off than another woman who would be your same height, but was much heavier.
This way, little petite people aren’t penalized and people that are overweight and really should be losing weight before they have this operation don’t kind of slide scot free and having the insurance cover their procedure or their operation.
I find personally that the scale is quite reasonable. And it seems to me, at least in my own brain, that that’s about the amount of tissue I would consider to be medically necessary to make this not a cosmetic operation.
How do we get insurance to cover this?
After I see you for your consultation, I will send a letter to the insurance company with a photograph and we detail your symptoms and your sizes and the amount of tissue that I expect to take off. And then they will contact both you and me and say yes or no.
If they say no then they nowadays have to tell us why they say no, and then we can look at their denial and determine whether or not there’s something you need to do to now meet the criteria. That could be well, let’s call your internist or your family practitioner and have them write for you to go to physical therapy for six weeks or have you come back in when your shoulder strap grooving is more involved.
If they say, well, you need to have 1000 grams off and I only thought you were going to have 500 grams off, and probably we’re not going to be able to make up that difference, and then this would be done on a cash-paid basis.
The History of Breast Reduction
A little bit about the history of breast reduction, because I always find history to be quite interesting. The earliest attempt to correct an enlarged breast was in 1670. The surgeon at the time had a patient that had sudden swelling of her breast. He put her on hot packs and different poultices of the time and then made an incision to try and get the swelling out but was completely unsuccessful.
It’s very interesting to me that the mention of this in historical tomes about surgery was in 1538 by Paulus of Aegina, but he wasn’t talking about a female breast, of course, he was talking about male breast enlargement, which is called gynecomastia.
At the time, they didn’t really care or even attempt to figure out a way to make a woman’s breast smaller. It was all about the fact that men had larger breasts, but they still couldn’t come up with an operation at the time that was successfully even make the male breast smaller.
In the early 1900s, European surgeons began attempts at breast reduction and it was mostly an amputative type of reduction. By that I mean they would just lop off the breast at the base and then sew it up. The breast has lots of blood vessels and of course they didn’t have the nice sutures like we have, anesthesia wasn’t like we have, they didn’t have cautery machine, and I would imagine that those operations were very bloody and there was a real risk that a woman could bleed to death from it.
Later on maybe 30 years later, they began the same amputative type of breast reduction surgery. But with these operations, they also were able to take the nipple and aeroeloa complex and remove it, and then take the tissue off from underneath and then sew it back onto the chest wall over the breast as a skin graft. And that’s still a very common way to do a breast reduction these days.
From the 1960s on as surgeons developed better understanding of the blood supply to the breast, and how to keep things alive, we began to have multiple techniques that actually left the nipple and aeroeloa attached to breast tissue and created a more aesthetically pleasing breast reducution at the end, so that the breasts didn’t look like it was lopped off and it didn’t look completely boxy.
Modern Breast Reduction Surgery
Nowadays, there’s three main ways to do a breast reduction.
1. Free Nipple Areola Graft
You can do like the older surgeons did what we call a free nipple areola graft that is done by removing the nipple areola complex as a little disk and then taking the tissue off from underneath of it till it’s very thin, reducing the breast and then figuring out where you want to have the new nipple and take the top of the skin off there. And then sew on this nipple areola complex that you removed as a skin graft and it will heal in and it actually looks just fine.
It doesn’t have any sensation though, and if you want to breastfeed, it’s not going to be possible because all of the ducks to the nipple have been cut.
But if it’s a patient that comes in who’s very large and possibly in poor health, let’s just say for example, she’s 75 years of age and her neck is just terrible from these large breasts and she’s got all kinds of medical problems, this would be a very efficient way to reduce the breast with very little risk.
I don’t tend to use it because I like to keep the nipples on for sensation. I also think that they look a little bit better when we keep them on. So this is an operative technique that I reserve only for very particular cases. But I do know lots and lots of surgeons, especially in our area, will do free nipple areola grafts because it’s a quick operation.
2. Superior Pedicle Technique
The other two techniques of breast reduction are based on how we keep blood supply to the nipple and areola because in these two techniques, we’re going to actually leave the nipple and areola still attached to breast tissue, and that can be done leaving it attached at the bottom or leaving it attached at the top. I am definitely a top person and that’s called superior pedicle because in this technique, we’re leaving and breast tissue all along the top and we’re removing the extra tissue which is very heavy at the base of the breast and out towards the armpit.
3. Inferior Pedicle Technique
In an inferior technique, you would remove breast tissue above the nipple and areola kind of going up towards under the collarbone. And then you can take some out from the side. I think these patients that have an inferior technique tend to all look flat at the top and pretty saggy and full out towards their armpit because you can’t get as much tissue off there as you would with a superior technique.
So why don’t all surgeons do a superior technique? Because it’s technically more challenging. It requires a lot more work to keep the nipple and areola on and keep it healthy and allow it to be rotated up to where it needs to go.
Unfortunately, in a podcast, there’s no way that I can show you how this operation is done. But when you come in the office, I do have pictures that will show you the superior pedicle technique.
I do want to clarify that there’s really nothing wrong with the inferior pedicle. I just can’t make it look as pretty as I can with a superior pedicle. So if you’re looking around for surgery, and you found one that you really like and they do inferior pedicle, there’s nothing wrong with it. I just can’t get it to look as pretty as I would like.
4. Liposuction for Breast Reduction (a largely abandoned procedure)
There’s one last technique to mention, although it’s been largely abandoned, and that’s liposuction in the breast for breast reduction. As we get older, our breast tissue becomes more fatty. And of course, as you get older, it really becomes more fatty. So it is possible to go in and actually liposuction fat out of the breast to reduce the volume. Of course, no skin is removed. So although you have a smaller breast, it’s going to be still in a bigger skin envelope, which would translate into the breast being flabbier and droopier.
It can also be an alternative for a woman if she says she just really doesn’t care and needs to have this operation done, in what I would consider a quick and dirty way, just like the free nipple grafting operation to me is a quick and dirty operation for breast reduction.
What to Expect Before, During and After Breast Reduction Surgery
First, the morning of surgery, I will meet you in the pre-op holding room. I’m going to mark on your breast. This shows me what skin I’m planning to take off, how high want to put the nipple areola complex because of course, we’re going to elevate the nipple. Otherwise, you’d still have a very droopy breast and the extent of the incisions and the placement of the incisions.
You would have an IV in. We would go back to the operating room, you would go on off to sleep. This is a general anesthetic so you’ll be totally asleep. During the operation, I’m going to have your arms out on arm boards. So you look sort of like you’re on a cross, and we will pad your arms very well.
I will have you sitting partially to all the way sitting up for most of the operation, and sometimes that puts a lot of pressure on the nerves as they come through the armpit and occasionally women will have mild tingling at their fingertips for a few days. If you have existing shoulder and neck issues, we have to talk about it because this really could be a problem.
For the actual technique, I’m going to cut around areola because normally we’ll make the areola size smaller. Nothing happens to the size of the nipple. We can’t make that change, and actually, it would be dangerous to do it, not dangerous to your health but the nipple probably wouldn’t survive if we tried to make the actual nipple smaller.
But most large breasts have a very large areola and we don’t want to finish your breast reduction and then have an areola that covers, like, 80% of the of the circumference of your breast.
So I have little cookie cutters – that’s actually what they are, little surgical cookie cutters, and various diameters – and I will pick a diameter that seems to be equivalent and compatible with your final breast size. If you have a real desire to have a larger or smaller nipple, then we can certainly talk about it and I’ll do what you want. Then I cut around the nipple and areola complex and above that, I’m going to take the top of the skin off and thin that tissue so that it can be rotated up into place.
Once the nipple and areola on the superior breast tissue is safely elevated, then breast tissue and skin are going to be removed and a large pie wedge from the central portion of the breast. And how thick and wide and tall and far I go will determine the final volume.
Also, breast tissue is removed along the base of the breast both to the inside and out laterally or towards the armpit. Especially out towards the armpit, lots of breast tissue is going to be removed.
Sometimes I will just cut this off and sometimes I’ll use liposuction and sometimes I use a combination of both of those. Once I’ve determined that I’ve taken off sufficient breast tissue, then the breast is going to be sewn together in the middle with multiple layers of stitches.
This helps to reshape the breast from a flat pancakey look to a nicer, more rounded look. We do shape pretty stringently, really tighten it up because as you breast heals and gravity occurs and the swelling goes out, then the nice round shape has a tendency to want to become less round and be a little saggy.
So after surgery, if you think “oh my gosh, she’s given me two volcanoes or two torpedoes here on my chest,” it was done on purpose because I know with time, those breasts are going to round out and be less full in all dimensions.
Breast Reduction Sizer Bra
The other thing that I use, which I think is a little different than most surgeons, is a Sizer Bra. And we do have a podcast on finding a Sizer Bra. This is just a bra that you get at the store (there’s a few more details about how to pick a bra), but let’s just say for purposes of discussion, you want to be in a 38 C.
So you’ve brought me a 38 C cup bra. I will sterilize it, and then as I’m reducing the breast, I will take the sterilized bra and put it onto your breast. Of course you’re sitting up to make sure that you’re filling it up the way that you want to. If you’re bulging out of that 38 C bra then I’m going to take more breast tissue out.
So I use this as a template to help me get the volume that you want. Even in a 38 C, for example, you could just fill the bra so that the bra material, the upper part of the bra goes down to your chest wall, or you could have a little bit of bulge at the top or you could really be spilling out, in which case you’re really a 38 D.
And those are the three delineations that we talked about, and you give me my marching orders on how you want to fill that particular bra. That way after surgery, very few people are disappointed with their size because they’ve actually chosen what they want to look like in terms of cup volume.
Very occasionally, I will have a patient where I need to keep the breast a little larger because I just need breast tissue left behind to keep everything healthy, or it’s impossible for me to get a pleasing shape without leaving it a little bit bigger. But I normally don’t veer off very much from what you’ve asked me to do.
The Breast Reduction Surgery Recovery Process
Once the internal suturing is done, then external stitches are put underneath of the skin and these will all dissolve. Usually there will be a drain which is a little plastic tube that goes under the skin and will come out through a little cut out towards your armpit and that will collect blood and serum from the interior part of the breast where I reduced and left essentially a little cavity so that that will all seal down.
Those drains normally come out second to third day and do not hurt. They are a nuisance. Nobody likes their drains, I am very much aware that you don’t want to have a drain and you don’t like it. But it is very helpful to allow you to heal more successfully and they’re not in for very long and they don’t hurt and I’m not gonna let you shower the first few days any which way so having a drain in is really just that: a nuisance.
Your dressings will be Steri strips, or little butterfly band aids all along the incisions, some gauze tape and then we put you in your postoperative bra which is not your Sizer Bra. This is just a front closure non-underwire bra that you will be wearing for the first week or two.
As you heal you can go into abroad of your own choosing, although I do ask you to please let me check it just to make sure it’s not going to compromise the incisions in any way.
Possible Breast Reduction Surgery Complications
What are some complications of breast reduction?
I’m just going to run through the major ones because there’s a whole laundry list that we discuss in your second discussion right before surgery, and it would take far too long to go over every one of them.
The biggest complication would be poor blood supply the nipple areola complex because we do base it on tissue and the blood supply. The blood has to flow down through that breast tissue and keep it alive. And sometimes it happens that a portion of the areola could die. A bad complication would be where the whole areola dies that would be very major and quite distressing, obviously to both my patient and to myself.
I can tell in the operating room if that nipple is struggling. I say nipple but I really mean nipple areola complex and there’s maneuvers that I can do such as resuturing or putting an ointment on that will dilate blood vessels.
But if it doesn’t seem to be doing well in surgery, I’m probably going to convert that to a free nipple graft so it will survive. But that would really be, to me the biggest and most serious complication.
Bleeding is always possible, but the blood vessels are easily taken care of with the electric cautery or will put stitches around the bigger veins. I don’t think I’ve actually had but maybe one or two patients with any bleeding issues after surgery where we’ve had to go back because of blood and we’ve needed to stop the bleeding and remove the collected blood.
The most common concern is how are your scars going to do?
Of course everybody heals differently when they scar and some people heal great and you can’t see the breast reduction scars at all. Others have a little thicker scar. And of course a bad scar would be a real ropey scar or one that is red and ropey and takes a year or two to become pale and flat.
If I had a crystal ball, the three things I would like to know: one would be how’s my patient going to scar. The second would be kind of guarantee that there’s going to be a good blood supply to the nipple areola complex.
And the third would be is she going to have good sensation in the nipple, because we have moved it up and sometimes you do lose sensation to your nipple when it’s stimulated. Sometimes you have more sensation, and sometimes you don’t have very good sensation to begin with, and then it’s better afterwards. But those would be the three things that I would really like to know.
Who is a Good Candidate for Breast Reduction Surgery?
So who’s a good candidate for breast reduction?
In my book is someone who is height/weight proportionate, so that you’re not too much overweight, Within maybe five or 10 pounds of ideal body weight. The breasts are large but the skin tone is good. You don’t have lots and lots of stretch marks. You’ve had your children and you’re done with breastfeeding.
That way I know when I reduce the breasts, it’s going to be a stable result, and it shouldn’t stretch too much afterwards. Stretch marks in the skin just show me that there’s not very good elasticity. In patients that have lots of stretch marks on the skin are always going to have droopier breasts no matter how much I tighten them when everything is said and done, because there’s just no elasticity. And there’s really nothing to do about that.
A poor candidate would be someone whose weight is not stable, who’s going up and down, because when they lose weight, their breasts will get smaller. And when they gain weight, they’re going to get bigger even after the surgery.
Really fatty breasts are hard to do, it’s just hard to give them any shape. Obesity is a huge problem for making a breast look good because usually the whole chest wall is thick, and there’s lots of fat going out towards the armpit and into the back rolls, and I can’t take care of that. So the breasts don’t look quite so pretty on a fat person with a fat breast as versus someone who’s not.
And then for a smoker, I actually will not do a breast reduction because the risk of wound healing problems and the nipple not surviving well are too high. So smokers for me are an absolute contraindication.
If you’re a bad diabetic and not controlled, or you have bad hypertension that’s poorly controlled, those of course, would be medical reasons not to do the operation. If you’re on a blood thinner, you would have to be able to be off the blood thinner. We could not do that on anticoagulation.
Young people are a relative contraindication. If a young woman comes in and she’s 18 or 19, and has very large breasts, I understand that she wants to have them reduced. But most often for a young person at that age, the breasts have not stopped growing.
So when I do a breast reduction, it is entirely possible that three or four years later, those breasts may continue to grow despite the operation because they’re getting hormonal stimulation to get larger. And so you could come back and say, “Gosh, I’m a cup size bigger than what I was after surgery.”
Some patients say well, let’s just knee jerk and we’ll just make the breasts really small in case I grew later, and that would be great – again, another crystal wall moment – if we knew you are going to continue to have breast growth. But what if you don’t know your breast is way smaller than what you want?
And of course you haven’t breastfed, so after we do this operation, I can’t guarantee you that you would be able to breastfeed. You might lose sensation, and then you’re a young person with scarring on your chest, which is a little easier when you’re older.
I think older women, we’ve had other operations, we’ve got stretch marks, we get the fact that there are scars, we’re not so worried that our partners gonna leave us because we have scars on her breast. But if you’re 20, and you have breast reduction scars in an intimate situation, that could be not so wonderful.
And these are things that we talk about in the discussion if it’s a young person coming in.
Breast Reduction Surgery and Breastfeeding
If you have not had children, can you breastfeed after a breast reduction?
I don’t know. We try and keep the nipple and areola attached to as much breast tissue as possible so that the ducts will still come up and you will be able to but there’s no way to know until you get pregnant and you try and breastfeed.
If you do breastfeed after a breast reduction, it’s probably going to alter your result because your breasts will be larger for lo those many months and when you stop breastfeeding, it’s probably going to be saggier and not look as good.
Most of my patients opt not to breastfeed, so they make a conscious decision that they are not going to breastfeed and have their breasts stretch out. But I have had many patients that have successfully breastfed.
Of course, if I could have a perfect patient, she would already be done with children and breastfeeding at the time of her operation.
What to Expect Postoperatively Following Breast Reduction Surgery
Postoperatively what should you expect?
There will be some pain. Sometimes it’s just discomfort and tightness because of course, all the tissue has been brought together and tightened, but most of the time, it really is pain, and we’re going to give you plenty of pain medicine for it.
The painful part is normally gone and just a few days and then it’s just tight and uncomfortable and less pain medicine or over the counter nonsteroidals like Advil will help quite a bit.
The breasts will be swollen, they don’t look like they’re going to for at least two to three months. It takes that long for the swelling to go down and the changes to occur so that they start to look more normal, more rounded and prettier.
It can take quite a bit of time for sensation to come back. Most often sensation starts back at about a week or two weeks with very aggravating little tingly electrical shocks, which is all a great sign.
Sometimes it can be two to three months before you start to get sensation back. And it can take up to a year and a half to know that you’ve gotten all or none of your sensation back depending on on how your body heals with this.
And then of course scars are very pink and noticeable for the first three months and begin to fade out and it could take four to 16 months for the scars to really fade and say “okay, this is what you look like.”
I tell patients final result is usually five to six months. Younger patients have much thicker breast tissue and it takes the whole time for that swelling to go down. Some of the older patients may look about like they’re gonna look in the four to five month time period.
Changes over time are really just growth in sagging. Sagging is because we live on a planet with gravity and there’s nothing you can do about that. The breast will be affected by gravity and it does start to pull it down and make it stretch. So wearing a bra is extremely helpful to counteract some of this.
Changes in your weight have a dramatic effect on your breasts. So if you gain 10 to 15 pounds, your breasts are going to get larger. If you lose 10 to 15 pounds, they’re going to get smaller. And then of course, we already talked about pregnancy and breastfeeding.
Conclusion
In plastic surgery circles breast reduction is the most positive patient operation. By that I mean, patients are just uniformly so happy that they did this operation.
It almost doesn’t matter if their scars are great or if they have feeling or if maybe the size is a little too big or too small. They’re just so happy that they did this and they feel so much better.
I always hear from patients, especially the older ones, “Why didn’t I do this 20 years ago and take the pain and the weight off my back and my shoulders, I would have been so much happier.”
So in that regards, that’s one of the reasons it’s my most favorite operation because I know that I’m making a direct and dramatic impact on someone’s life by doing this operation.
So that’s it for Episode Three, “Breast Reduction Surgery.”
I hope this has answered a lot of your questions. I think it will be very helpful to patients who are considering breast reduction because when you come in and we do our first consultation, it’s an awful lot of information to try and remember, and there’s no way you can write it all down.
And although we do provide you with consultation sheets, I don’t think they’re quite as informative as basically hearing me go over the entire consultation again.
If you have any questions at all, please call the office or look on our website, www.DrKerner.com and I hope you have enjoyed this presentation of “Breast Reduction Surgery.”
For other episodes, and upcoming episodes, you can go to my website www.DrKerner.com/podcasts or you can subscribe to our newsletter to know when a new episode is available. And this is also on YouTube.
Have a great day and don’t forget to use your sunblock.”