Elizabeth Kerner, MD
Plastic and Reconstructive Surgery

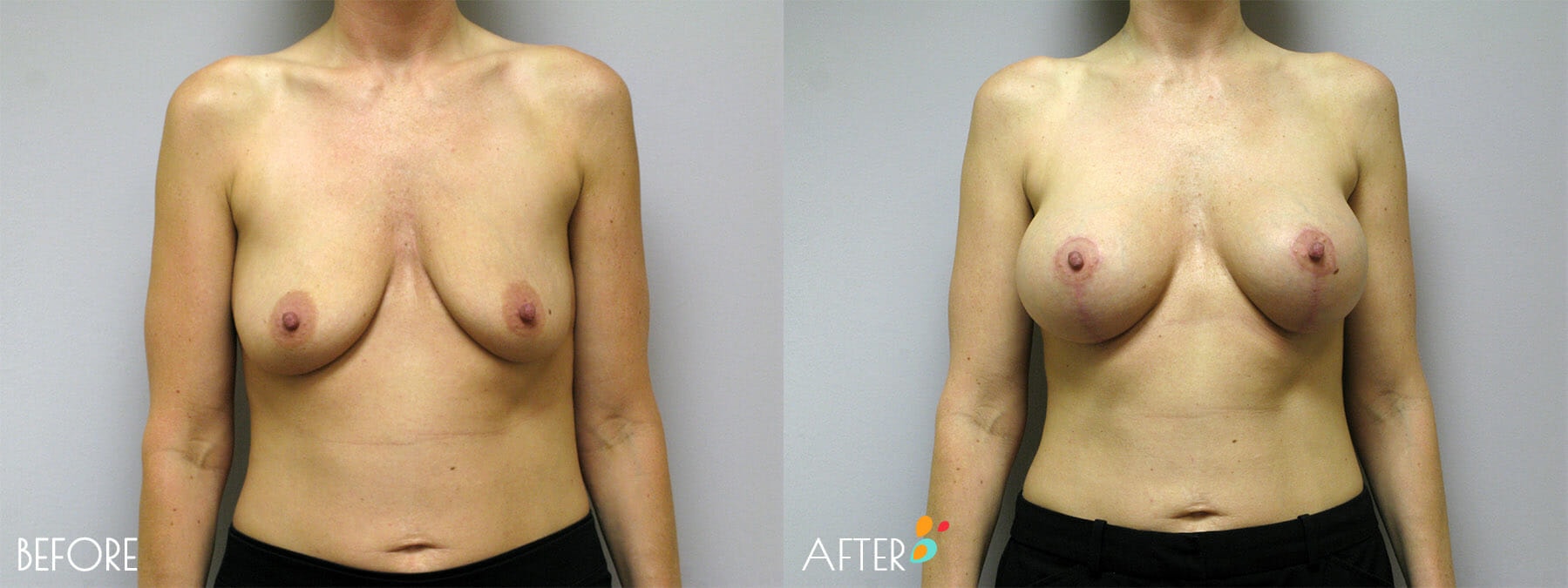
By removing loose, excess skin and tightening the breast tissue, the breasts are reshaped and better supported for a more attractive and youthful breast curvature and contour. In instances where there has been a significant loss in the volume of the breasts, implants may also be used to increase size and enhance the breast shape.
The degree to which breasts and nipples may sag or droop is affected by influences such as pregnancy, nursing, genetics and weight loss. In your private consultation, you and Dr. Kerner will discuss the condition of your breasts as well as the procedure and approach necessary to produce your desired outcome and restore your breasts to a more youthful and attractive shape and position.
“Welcome to Plain Talk About Plastic Surgery, a podcast that brings you down to Earth, honest and practical information about plastic surgery operations, procedures, and all the conditions that we deal with, based on my 32 years of experience as a plastic surgeon.
I’m Dr. Elizabeth Kerner, plastic surgeon based here in Plano, Texas, and today we’re going to talk about mastopexy.
What is a Breast Lift, also known as Mastopexy?
Mastopexy just means lifting of the breasts; “masto” being breast and “pexy” being lifting. I find the main point of confusion for most of my patients is: what is the difference between a mastopexy and a breast reduction, or a reduction mammoplasty?
There’s really very little difference. If you think about it, in a reduction we’re going to make the breasts smaller by removing more breast tissue. But you’re also going to have tightening of the skin envelope of the breast, which is exactly what happens in a lift, and also elevation of the breast gland on the chest wall.
So the only difference between the two is that in one, we’re going to take actual breast tissue out to purposefully make the breast gland smaller.
The first known articles about mastopexy occurred probably in the early 1920s. Surgeons in those days would take skin out around the areola to try and tighten up around the breast.
This is still done today and is called a periareolar or circumareolar mastopexy. I like to call it a doughnut mastopexy, and it’s done by just taking basically a doughnut-shaped circular amount of skin out around the areola to tighten and elevate it some. This works really well if you are just a little tiny bit droopy and the areola just needs to come up a small amount, certainly under an inch.
However, doing a doughnut mastopexy when you really need to elevate the nipple and areola multiple inches is going to cause all kinds of problems with wrinkling and flattening across the top of the breast mound.
When you come in for a consultation, I’ll show you pictures of what a doughnut mastopexy looks like. I think it does not respect the shape and boundaries of the breast and looks to me a little bit like chopping the top off of a mountain.
You just don’t have a nice, rounded, somewhat conical shape of the breast. And the wrinkles that result from the suturing, although people that do it say, “oh, it goes away,” I don’t think that it always goes away.
And oftentimes the sutures don’t hold and then the areola widens out and now you have a nicely lifted and tight breast with this kind of enormous areola taking up the whole top of it. That, to me, is not a very successful outcome.
Well, by the 1960s, plastic surgeons were doing what we do mostly now, which is what would be a lollipop or an inverted T incision. They did tend to elevate the skin off of the breast gland more than is done now, and that has all kinds of potential complications which I will discuss in a little bit.
Who is a Good Candidate for a Breast Lift?
Let’s talk about who’s a good candidate.
And even before I talk about that, I have to start by saying pretty much everybody is going to be a marginally good candidate. Because if you come in and you need a breast lift, then by default your breast skin is not very elastic, because if it had good elasticity, you wouldn’t have drooped. So logically, you’re kind of starting a little bit behind the eight ball.
A really good candidate for breast lift would be someone who has tight skin, and no stretch marks, and good firm breast tissue. She’s done with having children, is done with lactation, and her weight is ideal; there’s no more fluctuations. And of course, that individual usually has pretty good breasts because there was good elasticity to begin with and the breast gland is firm, so she wouldn’t be walking into my office asking for a breast lift!
So, if we back off just a little bit and say who’s a better candidate?
It would be a woman who has breast tissue, not completely fatty breasts, not really flabby breasts, that the stretch marks are fairly minimal, that the areola is not completely pointing down towards your toes, and of course, that your weight is reasonably stable.
Weight changes after a breast lift really ruin the operation because of the fluctuations up and down. I’m not talking about two to three pounds, but I am talking about the 10 to 15 pounds.
If you come in and talk to me and you want to lose 25 pounds, you really, really need to lose 20 of those 25 before you do a breast lift, because if you get motivated after your lift and you lose the 20 to 25 pounds, those breasts are going to deflate and sag again.
Who is a Poor Candidate for a Breast Lift?
Who’s a poor candidate?
Well, kind of the opposite of the marginally good candidate: someone whose breasts are completely full of stretch marks. It’s a very flat pancakey breast. There’s very little tissue. And I find women that have a very broad or sort of barrel chest where the breasts tend to slide off to the side – barrel is really the only way to describe it, there’s more fullness under the sternum – those breasts are really difficult to lift and make them look good.
When you don’t have much volume. It kind of doesn’t make sense to do a lift because what are you lifting? I mean, if you’re only going to lift an A cup, well, you don’t look a whole lot better.
Putting an implant in, of course, would be the issue at that point. Adding an implant in, which of course will give you volume is just a monkey wrench in the whole production. Because now you have more weight against the saggy skin envelope, which, although we’ve tightened, isn’t going to hold as well against more volume and strain of the implant because of the loss of elasticity.
Another whole issue is do you put the implant under the muscle or do you put the implant under the breast?
If you put it under the muscle, does it stay nicely under the muscle? And then as the breast tissue and skin loosens because of gravity and aging, does that skin envelope kind of fall off the bottom of the muscle, giving what we call a Snoopy Dog deformity (if you think of Snoopy’s nose – and if you think about it, you’ve seen lots of breasts that look like that)?
Or do you put the breast implant under the gland, where with gravity and aging and weight changes, it will all droop as one unit?
Those are very difficult decisions to make and there is not a one right answer at all for that.
Important Considerations for a Breast Lift
In a breast lift, you’re always going to lose volume because we’re taking skin out. If you don’t need skin removal, then you don’t need a breast lift.
So if you think about absolute volume in your bra, as I remove skin, you will have less absolute volume left. So when people say, I want to be a little smaller, that’s sort of a given.
If a woman comes in and says, “well, I want to lift and I want more volume,” then you’re always talking about having to do an implant with that.
Preoperatively, for me, I always request a mammogram because we need to know that there are no underlying issues with your breast tissue. Obviously, if you had a problem, you’d want to have that biopsy taken care of before you go down this route.
I would hate to take breast tissue out and find out, oh, you’ve got breast cancer and now everything you did has to be undone. And unfortunately, I do see a couple of breast cancers or significant atypical changes in the breast every year in patients that involve getting them introduced to a breast cancer surgeon and having closer surveillance or even a mastectomy down the road.
When you come in for a consultation, one of my first questions will be, “Is your weight stable?” And then we’ll talk about all the weight issues we talked about. And then “what volume do you want to be in?”
I need you to have in your mind what bra size you would like to fit in. So if you go back and listen to our podcast about sizer bras, I will ask you to bring in a bra that you would like to fit in. And then I determine with this sizer bra, are we looking at having to put an implant in to get to that, or do I need to take some breast tissue out to reduce your actual glandular tissue to fit into the size that you want?
Some women say, “I just want to keep whatever breast gland I have. That volume, whatever it might be, whether it’s B or C or D, that’s fine with me. Just keep it.” In which case then we don’t need to sizer bra.
The Breast Lift Operation
I do the operation in an operating room. I don’t have an in-office operating room. This is an asleep operation because I have you sitting up for the majority of the operation so that I can see what your breasts look like and make sure that the position on your chest wall is where I want it to be and that they’re symmetrical. Your arms will be out in a somewhat cross position. If you have carpal tunnel symptoms, sometimes that will exacerbate it, but it’s usually a very short lived problem.
The incision that I make: you’ll always have one around the areola, because we are almost always making the areola circumference smaller, and we’re lifting it up. That’s just a given in a lift.
So you always have a circular scar around the areola, and there’ll always be a vertical scar. This is taking out horizontal redundancy; so extra skin that goes across the base of your breast. For most of my patients, there’s going to be a scar in the fold, in your existing fold, because that’s taking out the vertical excess.
If your lift doesn’t need to be very much, you can get away with a lollipop, which is exactly what it sounds like. Around the areola and then vertical. But if you have a lot of extra skin to take out, if the lollipop (that vertical incision) is too long, it’s going to lengthen them with time and then your breast will bottom out. That’s when that scar stretches and the breast tissue sort of falls to the bottom of the breast and you look full and your areola tips up.
This is usually done as a day surgery operation. It will take me anywhere between three and four hours, or sometimes two and a half if you’re really small, sometimes four and a half if you’re quite big.
There is a lot of stitching, a lot of sitting up and laying down and sitting up again, trying to get you symmetrical. This is not just like a reduction. I can’t guarantee perfect symmetry, but we try and get mighty darn close. I like to say, as a patient told me, “they are sisters, not twins.”
Pain afterwards is usually not terrible. Tight, of course. A lot of tightness along the fold because of the suturing there. Breast tissue feels engorged; more than pre menstrual, not quite as bad as when your milk came in. Somewhere along those sorts of levels of pain.
Stitches will all be inside and dissolvable. We will use little butterfly bandaids called Steri-strips.
And then there’s a post operative bra, and you’re going to be wearing the post operative bra most of the time for about two weeks, and then you can go into light support.
My Thoughts on the Use of GalaFLEX in Breast Lifts
Internally, I do lots of suturing to help reshape the breast and to elevate it. I do know that some surgeons are using what’s called an acellular dermal matrix, or GalaFLEX, to put in and put this around the breast gland and tack it down to the muscle to try and create a shape and to hold it there.
It’s funny, back in the 60s, this elevation of the breast was done by putting stainless steel suture through the top part of the breast and around the rib. And it just didn’t work because the breast is basically a soft tissue and the wire would just usually pull on through the breast tissue.
So that didn’t work. It’s very much like thread lifts in a facelift. They don’t work for the very same reason: a permanent suture and soft tissue will always pull through.
GalaFLEX will eventually reabsorb. I suppose the way it works is to create scar. We don’t really want a whole lot of scarring in the breast because that could interfere with mammography.
And I think to put it in, you probably have to elevate the skin quite a bit, which means concerns about blood supply to the edges of the skin, which used to be a huge issue with a mastopexy but now because we don’t do that, is really not much of an issue.
So you’ve kind of gone backwards in terms of safety of the breast incisions and how they heal.
From this you can gather that I don’t do this. I have not seen any long term studies. I’ve seen lots of pictures at three to six months, but that’s way too short.
You really need to compare out at about three years. And a good study would do one breast with GalaFLEX and one breast without. And there, of course, have been no studies about that at all.
I am concerned about putting a foreign material into the breast. If you got infected, that would truly be a catastrophe.
And is it going to interfere with mammography?
For me? I don’t use GalaFLEX. I can’t tell you that it’s bad. I have lots of reservations on whether it’s good.
I am going to a meeting in a couple of weeks, and will be working with, actually, the vice President of the company who makes GalaFLEX.
And I intend to ask all these questions of that person, and hopefully will have more information to share after the meeting.
Breast Lift Postoperative Course, Risks and Recovery
Your postoperative course: you’ll go home. We do request that you not do a lot with your arms for the first week or two. So arms kind of down to the side and limit your lifting and picking up.
You will have Steri-strips over your incisions. Those will be changed every four to five days, and you’ll wear strips for about three weeks. And then you’ll begin scar massage.
It usually takes about three to six months for the scars to be pale. If you’re a really pink person, it could be nine months.
If you have a lot of pigmentation in your skin, you might get dark scars. And if you’re someone who makes very thick scars, then we really have to talk about whether this is the right operation for you.
After three weeks, generally, you can be back doing just about everything you want, with the exception of significant pectoral and latissimus work. So that would be pushups and pull ups and planks and burpees. By about a month to six weeks, you’re cleared for everything.
Sensation will take two weeks to three months to come in. Sometimes women will lose feeling in their nipples if they have to be elevated a great distance, but normally this is not as big a problem as it is in a reduction.
I would say the big risks with a mastopexy are whether you’ll keep your feeling, and how do the scars look, and then how well the breasts will stay elevated. There are lots of factors that the patient brings to the table, such as inelastic skin, flabby breast tissue, weight changes, that I can’t control.
So all of those things may cause your breasts to sag more after surgery than someone else’s.
Everybody settles a bit. So I make the breasts too high and a little too tight, a little too conical, because I know over about three to six months, those breasts are going to fall a bit, they’re going to round out, and have a more normal shape.
If I had to emphasize one point, It would be that gravity is always going to affect our breasts. So if you can be happier with a smaller breast, you’ll have less drop. Weight gain, weight loss, that cycle will affect the breast.
And, of course, pregnancy will hugely affect the breast. Doing a lift before pregnancy sort of doesn’t make any sense to me.
Implants, if you want more volume, certainly provide that. But again, you’re putting more weight on your breasts, and now you get into the whole gravity and stretching issue.
Many patients come in and they’re sort of an in-betweener. They’re a big lift or a small reduction.
For insurance purposes, if I’m taking enough breasts tissue out, we will call it a reduction. If I’m not taking enough breast tissue out, then it falls into the lift category. It doesn’t make a whole lot of difference to me whether I call it a lift or a reduction because it is essentially the same operation, just I’m going to take more breast tissue out in one versus the other.
Conclusion
That’s all I have for mastopexy.
Thank you very much for listening to this podcast. If you need more information, please give the office a call and we’ll be happy to answer any questions. Check out my Facebook page and our website, www.drkerner.com. That’s d-r-k-e-r-n-e-r .com.
We have lots of information about procedures there. We also send out regular newsletters with updates, and more importantly, inform you about upcoming specials. We just had a really big special over Christmas, and I think that was extraordinarily well received based on the number of people that called in to buy filler and Botox and other such things.
Thanks again for listening. Bye.”
The breast lift, or mastopexy, is an outpatient procedure that may take two to three and a half hours, depending on the degree of preoperative sagging and whether implants are used. Usually a patient can resume work within three to five days and may resume cardio-type exercise in about two weeks.